Obstructive Sleep Apnea (OSA) in children is a serious condition that can affect a child’s physical growth, behavior, and overall quality of life. It occurs when the airway becomes partially or completely blocked during sleep, causing breathing interruptions. Recognizing and treating pediatric Obstructive Sleep Apnea (OSA) early is crucial to prevent complications such as learning difficulties, poor school performance, daytime sleepiness, and even heart problems. This article discusses the most effective treatments for Obstructive Sleep Apnea in children, with a focus on adenotonsillectomy and Continuous Positive Airway Pressure (CPAP) therapy.
Causes of Obstructive Sleep Apnea (OSA) in Children
The most common cause of Obstructive Sleep Apnea (OSA) in children is enlarged tonsils and adenoids, which can block the upper airway during sleep. Other contributing factors include obesity, craniofacial abnormalities, neuromuscular disorders and genetic disorders.
Signs and Symptoms of Obstructive Sleep Apnea (OSA) in Children
Parents should watch for the following symptoms:
- Loud snoring
- Pauses in breathing during sleep
- Restless sleep or frequent awakenings
- Mouth breathing
- Daytime fatigue or hyperactivity
- Learning or behavioral issues
Diagnosis of Pediatric Obstructive Sleep Apnea (OSA)
Diagnosis typically involves a sleep study (polysomnography), which records brain activity, oxygen levels, heart rate, breathing patterns, and movements during sleep. This helps determine the severity of
Obstructive Sleep Apnea (OSA)and guides treatment.
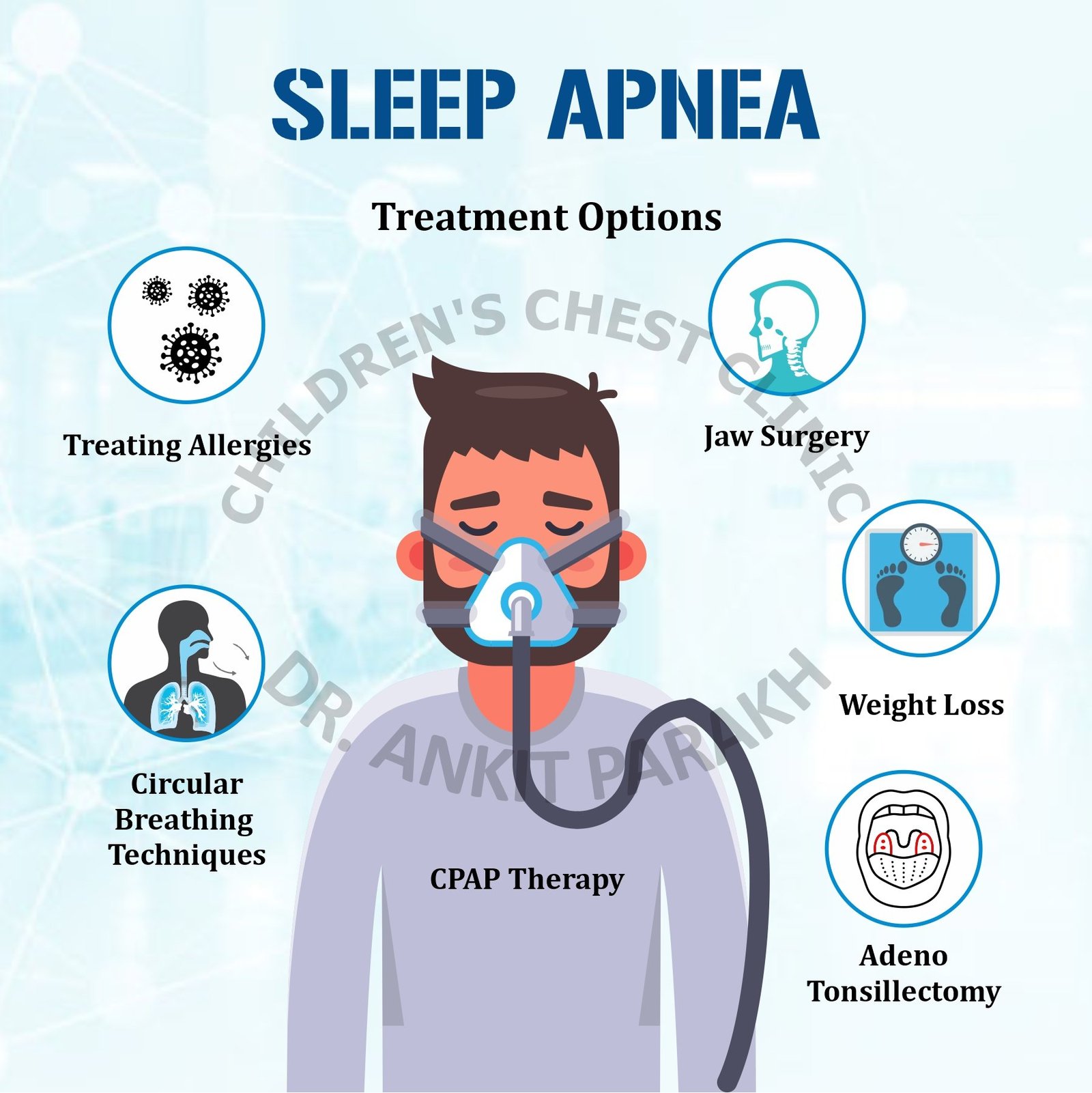
Treatment of Obstructive Sleep Apnea (OSA) in Children
1. Adenotonsillectomy – First-Line Treatment
For most children, the removal of enlarged tonsils and adenoids (adenotonsillectomy) is the first-line treatment for Obstructive Sleep Apnea (OSA). Studies show that this surgery can significantly improve or even cure Obstructive Sleep Apnea (OSA) in the majority of cases.
Benefits of Adenotonsillectomy:
- Restores normal breathing during sleep
- Improves behavior and school performance
- Reduces daytime sleepiness
- Enhances quality of life
The procedure is generally safe and performed under general anesthesia, with recovery usually within 1–2 weeks.
2. Continuous Positive Airway Pressure (CPAP) – For Persistent or Complex Obstructive Sleep Apnea (OSA)
If Obstructive Sleep Apnea (OSA) persists after adenotonsillectomy, or if surgery is not an option, CPAP therapy is recommended. CPAP involves wearing a mask over the nose or face during sleep. It provides a constant stream of air to keep the airway open.
Advantages of CPAP:
- Highly effective in managing Obstructive Sleep Apnea (OSA)
- Non-surgical
- Improves oxygen levels and sleep quality
3. Other Supportive Treatments
- Weight management in obese children
- Nasal corticosteroids or antihistamines for allergic causes
- Orthodontic treatment or surgery for craniofacial issues
Follow-Up and Long-Term Monitoring
Children with Obstructive Sleep Apnea (OSA) need regular follow-up to assess improvement in symptoms and adjust treatment if necessary. Repeat sleep studies may be needed to confirm resolution of Obstructive Sleep Apnea (OSA), especially if CPAP therapy is used or symptoms recur after surgery.
Obstructive Sleep Apnea (OSA) in children is treatable, and early intervention leads to remarkable improvement in health and development. Adenotonsillectomy remains the gold standard for most children, while CPAP therapy offers an effective alternative for persistent or complex cases. If your child shows signs of Obstructive Sleep Apnea (OSA), consult a pediatric sleep specialist for timely diagnosis and tailored treatment.
Conclusion
1. What age can a child have adenotonsillectomy for Obstructive Sleep Apnea (OSA)?
Adenotonsillectomy can be safely performed in children over 3-4 years old if they have significant symptoms of Obstructive Sleep Apnea (OSA) due to enlarged tonsils and adenoids. Adenotonsillectomy sometimes might be required in younger children having severe Obstructive Sleep Apnea (OSA).
2. Is CPAP therapy safe for children?
Yes, CPAP is safe and effective in children, but it requires proper fitting, regular use, and monitoring by a pediatric sleep specialist.
3. Can Obstructive Sleep Apnea (OSA) in children go away on its own?
In mild cases, OSA may improve as a child grows, but most moderate to severe cases require treatment to prevent complications.
4. How long does it take to see improvement after adenotonsillectomy?
Many children show noticeable improvement within days to weeks after surgery, especially in sleep quality and behavior.
5. What happens if Obstructive Sleep Apnea (OSA) is not treated in children?
Untreated Obstructive Sleep Apnea (OSA) can lead to serious consequences such as poor growth, learning problems, behavioral issues, and heart complications.